



















The free health care system was known for delays, caused in part by whittled-down funding. But Covid made waits for transplants, cancer treatments and other essential care even longer.
LONDON — Lara Wahab had been waiting for more than two years for a kidney and pancreas transplant, but months had passed without any word. So last month she called the hospital, and got crushing news.
There had been a good match for her in October, the transplant coordinator told her, which the hospital normally would have accepted. But with Covid-19 patients filling beds, the transplant team could not find her a place in the intensive care unit for postoperative care. They had to decline the organs.
“I was just in shock. I knew that the N.H.S. was under a lot of strain, but you don’t really know until you’re waiting for something like that,” she said, referring to the National Health Service. “It was there, but it sort of slipped through my fingers,” she added of the transplant opportunity.
Ms. Wahab, 34, from North London, is part of an enormous and growing backlog of patients in Britain’s free health service who have seen planned care delayed or diverted, in part because of the pandemic — a largely unseen crisis within a crisis. The problems are likely to have profound consequences that will be felt for years.
The numbers are stark: In England, nearly 6 million procedures are currently delayed, a rise from the backlog of 4.6 million before the pandemic, according to the N.H.S. The current delays most likely impact more than five million people — a single patient can have multiple cases pending for different ailments — which represents almost one-tenth of the population. Hundreds of thousands more haven’t been referred yet for treatment, and many ailments have simply gone undiagnosed.
There was already a huge and rising backlog of patients before the pandemic, but the unrelenting burden of the past two years, with health staff and hospital capacity stretched even thinner by coronavirus cases, saw it balloon to record proportions. The latest official figures are almost two months out of date, and experts say that severe staffing shortages this winter and the wildfire spread of the Omicron variant have almost certainly made the situation worse.
“Just because we’ve got Omicron doesn’t mean that other illnesses have just stopped still and don’t emerge and develop in people, sadly,” said Saffron Cordery, the deputy chief executive of N.H.S. Providers, a membership organization for health workers.
Public health experts worry that even if the pandemic eases and relieves some of the immediate burden, the pandemic and delayed care could do lasting harm to the health system, as well as patients.
This month, a report from the parliamentary health committee revealed a complex and troubling picture of record waiting lists, high caseloads and severe staffing shortages. It warned that a major expansion of the labor force was needed, but that the government was not doing enough to recruit and train health workers.
Generations of Britons have endured longer waits for treatment than many insured Americans, with most accepting that as the price of caring for everyone. But the problem has worsened for almost a decade, with critics accusing Conservative governments of steadily underfunding the system.
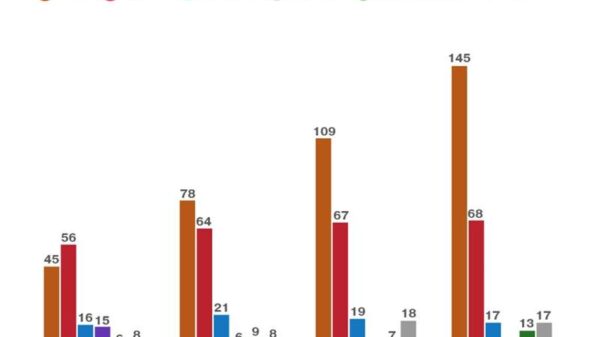
In 2012, there were 2.5 million cases awaiting specialist treatment in England. By the start of 2020, the backlog had swelled to 4.6 million cases, according to the N.H.S.
At the end of November 2021, the caseload was six million. More than 300,000 cases have been waiting for more than a year for planned care. A decade ago, there were fewer than 500.
The true backlog is probably much bigger, experts and government officials say. As the health committee noted in its report, the pandemic has greatly disrupted normal patterns of assessments and referrals by primary care doctors, keeping people off the official tallies.
A recent report from the National Audit Office estimated that there were 7.8 million to 9.8 million “missing” referrals — those that ordinarily would have occurred but never did — by primary care physicians from the start of the pandemic to September 2021, including 240,000 to 740,000 for suspected cancer cases.
“We are likely to see knock-on effects with people with other diseases, including but not limited to cancer, where treatment got delayed or postponed or we missed out on it,” said Peter English, a retired consultant in communicable disease control. “And they died because they didn’t have treatment they would otherwise have had.”
By the time the pandemic hit Britain, Ms. Wahab had been on the transplant list for months. In April 2019, her doctor told her that the Type 1 diabetes she has had since age 7 had left her with kidney failure and that her best chance at recovery was a simultaneous pancreas and kidney transplant.
Her doctors told her that it would take about six months to get onto the transplant list and then typically about a year to be matched with a donor.
But in the spring of 2020, overwhelmed hospitals across the country halted nonemergency care, including transplants, diverting staff to coronavirus response.
Since then, transplants have resumed and stopped, again and again. With each pandemic surge that filled intensive care units, the first treatments to be put on hold were planned procedures requiring intensive care beds — like transplants.
Because she has managed to stay off dialysis despite her worsening condition, Ms. Wahab is a more desirable transplant candidate because her likelihood of a positive outcome is better. But she is not sure how much longer she can hold on.
“It’s having a devastating effect on my day-to-day life,” she said. “I feel really hopeless going into 2022 — I’ve been waiting for this operation now for nearly three years.”
James Wilkinson, 46, was diagnosed with endocarditis, an inflammation of the lining of his heart caused by an infection that ate away at his aortic valve, and he had originally been booked for an operation in May 2020. The operation was canceled because of the pandemic. And then it was rescheduled and canceled three more times.
Mr. Wilkinson, who testified in front of a parliamentary committee late last year about his experience, said that he had eventually turned to private care to have the operation — something few people could afford.
“If it wasn’t for the private health care, we don’t know when my operation would have happened,” he said.
But it is not only those waiting for care they know they need who have been hurt. Cancer charities have warned that delays in diagnosing will also have devastating impacts.
Macmillan Cancer Support, a charity, estimates that some 50,000 people across Britain have not yet been diagnosed with some form of cancer that should have been caught earlier, in a direct result of the pandemic’s hindering screenings and referrals. The number of women being diagnosed with Stage 4 breast cancer — which means that the disease is advanced and very dangerous — has jumped by 48 percent in recent months.
Danni Moore, now 31, found a lump in her breast in early 2020, just before the pandemic. Ms. Moore, a mother to two children, was still breastfeeding her youngest and thought that she had a blocked milk duct. But her doctor referred her to a specialist clinic.
That appointment was canceled because of the pandemic. She rescheduled, but then had to cancel herself because her partner had contracted the virus and their household had to isolate.
“The knock-on effect Covid had has made everything much more difficult, and I had the lump way longer than I should have,” she said. “And it’s partly my fault. I should have gone much sooner, but equally hindsight is a wonderful thing.”
Ms. Moore said she put off making another appointment, and months went by. But then the lump grew, and in the spring of 2021, a year after she first found it, it was diagnosed as breast cancer. The months since have been an exhausting whirlwind of chemotherapy treatments and complications, which she has documented on her Instagram account.
While her treatment this year has continued without delay, and she credits the doctors and nurses with saving her life, she knows her initial diagnosis would have come sooner without the pandemic.
The surgery backlog has also influenced her decisions on what comes next. Ms. Moore has opted to have a double mastectomy, which is scheduled for early February. She said that she felt she could more readily live with having both breasts removed than having one removed and waiting an unknown length of time to have reconstructive surgery to reach a “new normal.”
“I have two young children,” she said. “I’ve already given up over a year to having cancer.”
She added: “I just don’t want to sit and just wait for another two or three and make this process longer than it ever needed to be.”













